Acid reflux happens when contents from your stomach move up into your esophagus. It is also called acid regurgitation or gastroesophageal reflux.
If you have symptoms of acid reflux more than twice a week, you might have a condition known as gastroesophageal reflux disease (GERD).
Symptoms and causes
Common signs and symptoms of GERD include:
A burning sensation in your chest (heartburn)
Chest pain
Chest pain
Regurgitation of food or sour liquid
frequent belching
Sensation of a lump in your throat
Laryngitis
Chronic cough
The lower esophageal sphincter (LES) is a circular band of muscle at the end of your esophagus. When it is working properly, it relaxes and opens when you swallow. Then it tightens and closes again afterwards.
Acid reflux happens when your LES does not tighten or close properly. This allows digestive juices and other contents from your stomach to rise into your esophagus.
GERD results in symptoms of heartburn and a sour taste in the mouth and can cause complications like Barrett’s esophagus and even esophageal cancer in the long run.
Some patients with GERD have hiatal hernia. Hiatal hernia is a condition where the upper part of the stomach called the fundus slides through the hiatus in the diaphragm into the thoracic region.
Conditions that can increase your risk of GERD include:
Obesity
Bulging of the top of the stomach up into the diaphragm (hiatal hernia)
Pregnancy
Delayed stomach emptying
Factors that can aggravate acid reflux include:
Smoking
Eating large meals or eating late at night
Eating certain foods (triggers) such as fatty or fried foods
Drinking certain beverages, such as alcohol or coffee
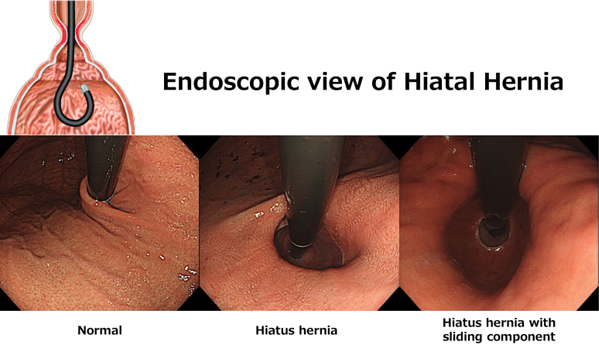
Hiatal Hernia
A hiatal hernia is when your stomach bulges up into your chest through an opening in your diaphragm, the muscle that separates the two areas. The opening is called the hiatus, so this condition is also called a hiatus hernia.
Ordinarily, your esophagus goes through the hiatus and attaches to your stomach. In a sliding hiatal hernia, your stomach and the lower part of your esophagus slide up into your chest through the diaphragm. Most people with hiatal hernias have this type.
*These endoscopic pictures are looking at the gastric cardia which are taken in endoscopic retroflex position
Diagnosis and Tests
Upper endoscopy
Your doctor inserts a thin, flexible endoscope down your throat, to examine the inside of your esophagus and stomach. Test results can often be normal when reflux is present, but an endoscopy may detect inflammation of the esophagus (esophagitis) or other complications. An endoscopy can also be used to collect a sample of tissue (biopsy) to be tested for complications such as Barrett’s esophagus.
Esophagogram (Esophageal barium swallow)
X-rays are taken after you drink barium that coats and fills the inside lining of your digestive tract. The coating allows your doctor to see a silhouette of your esophagus and stomach. Esophageal motility disorders can be diagnosed with this test.
Esophageal 24hour pH testing
A monitor is placed in your esophagus to identify when, and for how long, stomach acid regurgitates there. The monitor connects to a small computer that you wear around your waist or with a strap over your shoulder. The monitor is a thin, flexible tube (catheter) that’s threaded through your nose into your esophagus.
Test results can help your physician determine:
Whether or not your symptoms are related to GERD
How your GERD symptoms respond to your current therapy
If your stomach acid is reduced enough to control your present symptoms
Whether your upper respiratory symptoms are related to acid exposure
Whether or not you are a candidate for alternative medical or surgical management.
Esophageal manometry
This test measures the muscle contractions in your esophagus when you swallow. Esophageal manometry also measures the coordination and force exerted by the muscles of your esophagus.
Endoscopic pressure study integrated system:EPSIS[1,2]
Endoscopic pressure study integrated system (EPSIS) has been developed at our center to assess the function of lower esophageal sphincter (LES). EPSIS can be used as an ancillary diagnostic tool to diagnose acid reflux.
EPSIS allows to monitor an intragastric pressure (Pressure inside the stomach) while inflating the stomach during gastroscopy. Endoscopic evaluation of air valve mechanism of LES function can be achieved.
This study only takes approximately 5 minutes during gastroscopy and is considered very safe with minimal discomfort. No adverse events have been experienced.
Treatment options for GERD
Medications
The first-choice treatment for GERD is anti-acid medication, usually a Proton Pump Inhibitor (PPI).
Proton pump inhibitors include esomeprazole, lansoprazole, omeprazole, and rabeprazole. Vonoprazan is also available in Japan. Although generally well-tolerated, there are some complications related to chronic use.
When PPIs are ineffective, anti-reflux surgery (such as laparoscopic Nissen fundoplication) is generally recommended; however, many patients would prefer to avoid surgery.
ARMA: A novel endoscopic treatment for GERD
What is ARMA(Anti-reflux mucosal ablation)?
ARMA is a novel, minimally invasive endoscopic treatment for GERD. [3]
Antireflux mucosal ablation (ARMA) is a modified antireflux procedure that arises from our experience with ARMS.
In 2014, Dr.Haruhiro Inoue has developed ARMS “Anti-reflux mucosectomy”. This is an incisionless endoscopic GERD treatment achieved by mucosectomy of the mucosa at the gastric cardia. By ARMS, the gastro-esophageal flap remodels into an effective anti-reflux valve during the healing process.[4,5]
ARMA is a modified procedure of ARMS which artificial ulcer is created by “Ablation” instead of “Mucosectomy”.
Mucosal ablation by Argon plasma coagulation (APC) shows scar formation at the gastric cardia similar to the scarring seen with resection and results in narrowing of the cardiac opening, resolving reflux. (see pictures below)
Anti-reflux effect will be seen usually after 1-2 months after the procedure, when the artificial ulcer heals, and scarring process finalizes.
Our study shows that ARMA resolves reflux symptoms, improves quality of life, reduces or eliminates medications, and decreases acid exposure in patients with chronic GERD.
The ARMA procedure has been presented at Digestive Disease Week (DDW), and published in peer-reviewed international scientific journals.
The ARMA procedure has been approved by the Ethics Board of Showa University Koto-Toyosu Hospital.
Endoscopic view Before and After ARMA
Before: Endoscopy in retroflexion demonstrated significant hiatal hernia but no sliding component. Immediately post-ARMA: Endoscopy in retroflexion showed artificial ulcer in “horseshoe shape.” After 2 months: Mucosal flap valve was re-shaped. Anti-reflux effect is expected as a result of narrowing the cardia.
Indication for ARMA
Patients who do not respond to medications for GERD.
Patients who would prefer to avoid taking long-term medications for GERD
Presence of esophageal or extra-esophageal complications of GERD
Presence of hiatal hernia
Refractory GERD after abdominal surgery (i.e: post-gastrectomy, including sleeve gastrectomy)
Benefits of ARMA
Ablation treatment – no surgery or implants
Minimally invasive
Takes only around 30 minutes
Most of the patients will benefit from single time procedure, although ARMA is repeatable
No major complications
Surgical treatment for GERD
In most cases, lifestyle changes and medications are enough to prevent and relieve symptoms of GERD. But sometimes, surgery is needed.
Laparoscopic anti-reflux surgery for GERD may involve a procedure to reinforce the lower esophageal sphincter, called Nissen fundoplication. In this procedure, the surgeon wraps the top of the stomach around the lower esophagus after reducing the hiatal hernia, if present. This reinforces the lower esophageal sphincter, making it less likely that acid will back up in the esophagus.
(Figure 2)
In a Nissen fundoplication, also called a complete fundoplication, the fundus is wrapped the entire 360 degrees around the esophagus.
GERD care at Showa University Koto Toyosu Hospital
Your GERD CARE team
Showa University Koto Toyosu Hospital, Digestive Diseases Center GERD care team includes doctors trained in digestive diseases (gastroenterologists) and surgeons who work together to provide exactly the care you need.
Having all of this subspecialized expertise in a single place, focused on you, means that you’re not just getting one opinion — care is discussed among the team, and highly specialized GERD experts are all working together to determine what’s best for you.
We know that frequent acid reflux, chronic heartburn, and other GERD symptoms can negatively affect your quality of life.
If you are suffering from GERD and medication is not providing relief, we can help.
【References】
Inoue H, Shimamura Y, Rodriguez de Santiago E et al. Diagnostic performance of the endoscopic pressure study integrated system (EPSIS): a novel diagnostic tool for gastroesophageal reflux disease. Endoscopy 2019; 51: 759-762
Iwaya Y, Inoue H, Rodríguez de Santiago E et al. Endoscopic pressure study integrated system reflects gastroesophageal junction competence in patients with erosive esophagitis and Barrett´s esophagus. Dig Endosc 2020, DOI: 10.1111/den.13644:
Inoue H, Tanabe M, de Santiago ER et al. Anti-reflux mucosal ablation (ARMA) as a new treatment for gastroesophageal reflux refractory to proton pump inhibitors: a pilot study. Endoscopy international open 2020; 8: E133-e138
Inoue H, Ito H, Ikeda H et al. Anti-reflux mucosectomy for gastroesophageal reflux disease in the absence of hiatus hernia: a pilot study. Annals of gastroenterology 2014; 27: 346-351
Sumi K, Inoue H, Kobayashi Y et al. Endoscopic treatment of proton pump inhibitor-refractory gastroesophageal reflux disease with anti-reflux mucosectomy: Experience of 109 cases. Dig Endosc 2020, DOI: 10.1111/den.13727: